DUPLEX SCANNING VERSUS
ANGIOGRAPHY IN THE ASSESSMENT OF
CAROTID ARTERY
STENOSIS
Comment. The following paper was never published and the specific issue examined in this article (ultrasound versus angiography)
is rapidly becoming superseded. Many vascular units have adopted a Duplex
only policy on the basis of its reported accuracy in the literature. For
some units it is impossible to make a meaningful comparison of Duplex and
angiography because of relatively small numbers of procedures. Many units,
contrary to all recommendations in the published literature, have just not
bothered to perform a comparison and rely instead on published Duplex criteria
which may not be applicable. Despite these developments, the more general point made in the article
regarding the variablility and inherent operator variation of Duplex ultrasound
still stand. A recent consensus statement from the Society of Radiologists
in Ultrasound (Grant EG et al, 2003) has
highlighted these issues (as shown in the graph) and made recommendations
regarding the ultrasound assessment of carotid stenosis. 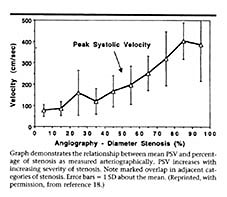
Recent UK recommendations are that patients should have two ultrasound scans or an ultrasound scan and an MRA prior to surgery to ensure an accurate estimate of stenosis has taken place.
The recent clarification of the role of carotid endarterectomy in asymptomatic carotid disease also places more pressure on angiography, because of the small but definite risk attached to performing an invasive procedure. Some form of confirmatory investigation is advisable and Magnetic Resonance Angiography (MRA) and CT angiography both give good information. At present I use Duplex in conjunction with CT angiography to assist in decision making for patients with carotid artery disease.
S Subramanian FRCS, Senior House Officer in Surgery
J Henderson FRCR, Consultant Radiologist
MX Gannon MD FRCS, Consultant Surgeon
M Goldman MD FRCS Consultant surgeon
DA Mosquera MD FRCS Consultant Surgeon
Birmingham Heartlands Hospital, Birmingham B9 5SS
INTRODUCTION
METHODS
RESULTS
DISCUSSION
REFERENCES
ABSTRACT
Duplex scanning has been proposed as a non-invasive alternative to preoperative angiography for patients with carotid artery disease. The aim of this study was to determine the degree of agreement between Duplex and angiography in the assessment of carotid artery stenosis by analysing the symptomatic and asymptomatic arteries separately.
A review of radiology reports from 73 patients undergoing both Duplex and angiographic assessment of carotid artery stenosis was performed.
In the symptomatic artery the agreement rate was 84.9% (62 of 73) with a kappa value of 0.63 (95% confidence intervals 0.42-0.83). Combining results from both carotid arteries falsely elevated agreement rates to 87.1% (kappa = 0.79, 95% CI 0.70-0.88). Disagreement between Duplex and angiography could have led to inappropriate surgery in 15.1% (n=11) of patients.
Combining asymptomatic and symptomatic carotid arteries from the same patient for the purposes of analysis is invalid and may artificially elevate agreement rates. High agreement rates between Duplex and angiography may mask important clinical discrepancies.
The management of symptomatic carotid artery disease is based on rigorous clinical studies in which angiographic assessment of internal carotid artery stenosis has defined the patients likely to benefit from endarterectomy1,2.
Angiography is an invasive procedure which carries a small risk of local complications at the arterial puncture site, and the more serious risk of stroke. Duplex scanning has been proposed as a non-invasive alternative and some surgeons already operate routinely on the basis of Duplex findings alone3. Although there is a potential saving both in complications and expense, Duplex scanning is highly operator-dependent and even its proponents recommend laboratory specific comparison of Duplex and angiography prior to abandoning preoperative carotid angiography4,5. Duplex may provide an accurate assessment of carotid artery stenosis, but was not used in the ECST or NASCET trials to classify carotid artery disease prior to surgery. If Duplex is to stand alone as a pre-operative investigation, then it must demonstrate high agreement rates with angiography and must be able to match the accuracy of angiography in selecting patients for endarterectomy.
Most previous comparative studies of Duplex and angiography have combined figures from both the asymptomatic and the symptomatic carotid arteries in the same patient to determine agreement rates. This seems inappropriate and may be incorrect on statistical grounds because it combines assessments within individuals and assumes they can be treated as independent observations, analogous to measurements on different patients.
The aims of this study were firstly to determine the degree of agreement between Duplex scanning and digital subtraction angiography in patients with symptomatic carotid artery disease, and secondly to analyse the symptomatic and asymptomatic arteries individually to determine the effect on agreement rates.
We performed a retrospective review of Duplex and angiography reports on patients with symptomatic carotid artery disease, presenting to vascular surgeons at Birmingham Heartlands Hospital between April 1995 and December 1997. Only patients with both Duplex and angiography reports were included, but unit policy is for all patients to undergo both investigations prior to endarterectomy. Ambiguous reports were excluded. The symptomatic artery was the carotid artery responsible for the patients symptoms, and the opposite artery the asymptomatic side.
We recorded the degree of stenosis for each carotid artery as indicated by both the Duplex and angiography reports for each patient. Stenoses were classified into groups similar to those used in recent trials1,2. The groups were mild disease or normal (0-29% stenosis), moderate disease (30-69% stenosis), severe disease (70-99% stenosis) and occluded. If the Duplex or angiography report indicated a range of possible stenosis that straddled these grades, classification was on the highest figure in the range.
Duplex scanning was performed by three different consultant radiologists and one vascular technologist all experienced in the use of vascular ultrasound. Scanning was performed on the HDI ATL Ultramark 9 and the HDI ATL 3000 machines. Duplex grading of stenoses was performed using peak systolic velocity measurements at the site of maximum stenosis using published criteria6 (see table 1). Angiographic classification of stenoses was performed after selective digital subtraction angiography with at least two different views of the carotid bifurcation. Assessment of carotid stenosis on angiography used North American trial methodology1, with as the denominator the diameter of the distal normal internal carotid artery. Actual assessments varied between radiologists from caliper measurements to eyeball estimation.
| Diameter classification Peak systolic velocity | |
| 0-39% | <110 cm/s |
| 40-59% | 110-150 cm/s |
| 60-79% | 150-250 cm/s |
| 80-99% | 250-615 cm/s |
| 99%+ | Extremely low |
| 100% (occluded) | No flow |
Table 1 Duplex criteria for grading carotid stenosis
Kappa values were used to assess the degree of agreement between Duplex and angiography. The results for the symptomatic and asymptomatic internal carotid arteries were analysed separately and in combination.
Seventy three patients underwent both Duplex scan and angiography for the assessment of symptomatic carotid disease. There were 48 male patients and the mean age of presentation was 65 years (range 43-87 years). No major or minor cerebrovascular events or local complications were recorded as a result of angiography.
On the symptomatic side, the majority of stenoses fell into the severe or occluded group (59 of 73, 80.8%). On the asymptomatic side, the majority of stenoses fell into the mild or moderate group (51 of 67, 68.7%; see tables 2 and 3). Statistical proof that the symptomatic and asymptomatic arteries are different populations requires testing of the null hypothesis (see table 4). If the null hypothesis is correct there should be no difference in the disease distribution between the two internal carotid arteries in the same patient. The highly significant Fishers exact test based on table 4 indicates that the null hypothesis can be rejected and that the arteries should be treated as two different populations for the purposes of analysis.
The results of the comparison for the symptomatic internal carotid artery are shown in Table 2. Perfect agreement between Duplex and angiography was seen in 4 patients with mild disease, 2 patients with moderate stenosis, 50 patients with severe stenosis and 6 patients with an occluded vessel. The overall agreement rate was 84.9% (62 of 73 patients) with a kappa value of 0.63 (95% confidence intervals 0.42-0.83). Sensitivity for severe stenoses was 92.6% (50 of 54 correctly identified) with a specificity of 63.2% (12 of 19 correctly identified).
Four patients with severe stenosis on Duplex had only moderate disease on angiography and three patients with occluded vessels at angiography had severe stenosis on Duplex. These patients might have undergone unnecessary surgery. Four patients with mild or moderate disease on Duplex had severe stenosis on angiogram and these patients might have been denied a potentially beneficial operation. Discrepancies between Duplex and angiography (11 patients,15.1%) may adversely affect subsequent surgical management.
The results of the comparison for the asymptomatic internal carotid artery are shown in Table 3. There were 67 patients with acceptable reports. Of these 58 showed perfect agreement between Duplex and angiographic grading with an agreement rate of 86.6% and a kappa value of 0.77 (95% confidence intervals 0.63-0.91). Sensitivity for severe stenoses was 87.5% (14 of 16 correctly identified) with a specificity of 94.1% (48 of 51 correctly identified).
If the results from both internal carotid arteries are combined this gives a total of 140 vessels for comparison and would artificially elevate the agreement rate to 87.1% with a kappa value of 0.79 (95% CI 0.70-0.88). This is much better than for the symptomatic artery alone (kappa 0.63, 95% CI 0.42-0.83) and with closer confidence intervals providing a spurious validity to the result.
| ANGIOGRAM | ||||
| Mild | Moderate | Severe | Occluded | |
| Mild (0-29%) | 4 | 2 | ||
| Moderate (30-69%) | 2 | 2 | ||
| Severe (70-99%) | 4 | 50 | 3 | |
| Occluded | 6 | |||
Table 2: Comparison of Duplex and angiogram findings in the symptomatic internal carotid artery (Agreement rate 84.9%, 62 of 73,k = 0.63).
| ANGIOGRAM | ||||
| Mild | Moderate | Severe | Occluded | |
| Mild (0-29%) | 35 | 2 | 2 | |
| Moderate (30-69%) | 2 | 7 | ||
| Severe (70-99%) | 1 | 2 | 14 | |
| Occluded | 2 | |||
Table 3: Comparison of Duplex and angiogram findings in the asymptomatic internal carotid artery (Agreement rate 86.6%, 58 of 67,k = 0.77).
| SYMPTOMATIC SIDE | ||
| ASYMPTOMATIC SIDE | >70% stenosis | <70% stenosis |
| >70% stenosis | 14 | 0 |
| <70%stenosis | 39 | 14 |
Table 4: Comparison of disease distribution in the symptomatic and asymptomatic carotid arteries (Fishers exact test using predicted values versus observed, p<0.0001).
In this study the agreement rate between Duplex scanning and angiography in the investigation of symptomatic carotid artery disease was high at 84.9%. This is comparable with other larger studies7,8,9, but the poor agreement in 15.1% (11 of 73 patients) could have led to incorrect surgical management in all cases. Combining results from both carotid arteries did improve the agreement rate, but is invalid because the distribution of disease is significantly different in the symptomatic and asymptomatic internal carotid arteries (as shown in tables 2, 3 and 4).
The demonstration of a different and more severe distribution of carotid disease in symptomatic when compared with asymptomatic arteries is not surprising or original1, but its importance has been ignored previously. Previous studies examining agreement rates between Duplex and angiography have not accounted for the statistical relevance of this different disease distribution and have performed invalid calculations of agreement rates based on combined figures from both the symptomatic and asymptomatic arteries. As we have demonstrated this can lead to a bias in favour of increased agreement between Duplex and angiography. Previous work demonstrating high agreement rates may have lead to a systematic bias in the literature favouring Duplex only protocols and may need to be re-evaluated in the light of these findings.
Radiology reports alone were used to grade carotid stenosis and ambiguous reports were excluded. These exclusions are likely to improve the agreement rate, as difficult cases in which discrepancies may have been present were excluded from analysis. Duplex scanning was performed by four operators on two machines. Restriction of scanning to one operator on a single dedicated machine and a review of radiological findings may have improved agreement rates, but would probably not be representative of practice in most hospitals. This is important because the results of Duplex scanning from academic centres, as part of prospective studies with standardised reporting from single operators, may not be transferrable to wider surgical practice.
Our findings are supported by other studies. Bain et al5 in a study of 272 patients confirmed a degree of agreement between angiography and Duplex higher than ours at 89%, but still concluded that angiography provided additional information in 89 patients and in 26 patients surgery was not performed because of information obtained from angiography. Investigators in the NASCET trial were hesitant to recommend surgery on the basis of Duplex findings alone because of the high number of false positive scans10 and also commented that it was unclear whether measurements obtained by ultrasonography or other noninvasive methods could be substituted for those based on angiography1. A recent review in the British Medical Journal has also concluded that angiography is an essential prerequisite prior to surgery11.
Other authors do recommend a Duplex only policy on the basis of their personal results, and report that this is safe3,12. Safety is important, but not as important as the appropriateness of endarterectomy. In one study13 the authors showed that a peak systolic velocity of 130cms/sec was 96% sensitive in detecting a 70% or greater stenosis. If surgery had been performed on this basis, over 33% of patients would have had inappropriate operations because of the poor specificity. Duplex specificity can be improved by raising peak systolic velocity criteria, but at the risk of excluding some patients with treatable disease by lowering the sensitivity. Duplex criteria themselves are not necessarily transferrable between centres as technology itself also affects measurements. Thrush et al14 have reported up to 60% errors in peak velocity measurements, which were machine dependent, and data from ACAS15 indicate that only 21% of Duplex machines attained acceptable sensitivity for the prediction of a 60% stenosis. Duplex also has specific anatomical limitations, such as inability to assess the carotid siphon or aortic arch.
Widespread adoption of a Duplex only policy may not affect the safety of surgery, but would make it impossible to guarantee its appropriateness. In the light of rigorous trials using angiography to define appropriate patient groups for endarterectomy it seems premature to recommend widespread adoption of a Duplex only policy. Until the accuracy and reproducibility of Duplex between centres improves, the preoperative investigation of choice should remain angiography.
1. The North American Symptomatic Carotid Endarterectomy Trial
Collaborators. Benefit of carotid endarterectomy in patients with symptomatic
moderate or severe stenosis. N Engl J Med 1998;339:1415-25.
2. Randomised trial of endarterectomy for recently symptomatic
carotid stenosis: final results of the MRC European Carotid Surgery Trial.
Lancet;351:1379-87.
3. Loftus IM, McCarthy MJ, Pau H et al. Carotid endarterectomy without
angiography does not compromise operative outcome. Eur J Vasc Endovasc Surg
1998;16:489-493.
4. Hood DB, Mattos MA, Mansour A et al. Propsective evaluation of new Duplex
criteria to identify 70% internal carotid artery stenosis. J Vasc Surg
1996;23:254-262.
5. Curley PJ, Norrie L, Nicholson A, Galloway JMD, Wilkinson ARW. Accuracy of
carotid Duplex is laboratory specific and must be determined by internal audit.
Eur J Vasc Endovasc Surg 1998; 15: 511-514.
6. Sanders RC. Clinical sonography. 2nd edition, Little, Brown and Co. 1991
p384, table 39-1.
7. Blakeley DD, Oddone EZ, Hasselblad V, Simel DL, Matchar DB. Noninvasive
carotid artery testing. A meta-analytic review. Ann Intern Med 1995;122:360-367.
8. Bain DJ, Fergie N, Quin RO, Greene M. Role of arteriography in the
selection of patients for carotid endarterectomy. Brit J Surg 1998;85:768-770.
9. Hood DB, Mattos MA, Mansour A et al. Propsective evaluation of new Duplex
criteria to identify 70% internal carotid artery stenosis. J Vasc Surg
1996;23:254-262.
10. Haynes RB, Taylor DW et al. Poor performance of Doppler in detecting high
grade carotid stenosis. Clin Res 1992; 40:184A.
11. Barnett HJM, Eliasziw M, Meldrum HE. Prevention of ischaemic stroke. BMJ
1999; 318: 1539-1543.
12. Shifrin EG, Bornstein NM, Kantarovsky et al. Carotid endarterectomy
without angiography. Brit J Surg 1996;83:1107-1109.
13. Curley PJ, Norrie L, Nicholson A, Galloway JMD, Wilkinson ARW. Accuracy
of carotid Duplex is laboratory specific and must be determined by internal
audit. Eur J Vasc Endovasc Surg 1998; 15: 511-514.
14. Thrush AJ, Evans DH. Intrinisic spectral broadening: a potential cause of
mis-diagnosis of carotid artery disease. J Vasc Invest 1995;1:187-192.
15. Howard G, Baker WH, Chambless LE, Howard VJ, Jones AM, Toole JF et al. An
approach for the use of Doppler ultrasound as a screening tool for
hemodynamically significant stenosis (despite heterogeneity of Doppler
performance). Stroke 1996;27:1951-1957.
16. Grant EG et al. Carotid artery stenosis:
gray-scale and Doppler US diagnosis - society of radiologists in ultrasound
consensus conference. Radiology 2003; 229: 340-346.
![]() Bookmark this on Delicious
Bookmark this on Delicious  reddit
reddit 
![]() facebook
facebook
Last updated Saturday, 13 March, 2010 7:21 PM